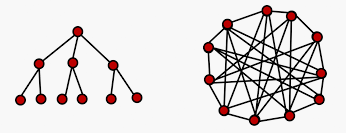
Centralised vs. Decentralised Decision Making
The UK Government’s failure to achieve its target of 25,000 tests per day for Covid-19 provides an excellent case study on the differences and impact of centralised vs. decentralised working and decision making. Whilst accepting there might be a problem with the sourcing of reagent chemicals for the DNA testing, according to a former director of the World Health Organisation we are not making the most of the opportunities currently available to us.
Public Health England (PHE) want to control who can do the tests, and until quite recently only allowed PHE labs to do the testing. Apparently there are 44 molecular virology labs in the UK, none of them working at capacity and few who have been approved for Covid-19 testing. If they were each doing 400 tests a day we would be at the same level of testing as Germany
Centralised control does ensure quality and standards, but surely these can be relaxed in the interests of rapidly ramping up testing. Quality could thereafter measured and controlled by PHE using statistical sampling techniques. There would also be an opportunity for this network of labs to share best practice.
Networks may not deliver a gold standard from day one, but knowledge sharing between them would get them there quickly, and (I would argue) quicker than communication being controlled and managed through a centralised authority. In the mean time, we’ve got thousands of NHS workers not able to work because they haven’t been tested. Time I think for the UK Government to start decentralising their decision making processes in the interest of speeding up critical interventions.
Previously posted as a comment to The Obvious? blog.









One thought on “Centralised vs. Decentralised Decision Making”
This is mind blowing, thanks for sharing this valuable content.